
Enkephalins are endogenous pentapeptides involved in regulating pain sensation (nociception). Structurally, the enkephalins are pentapeptides that are distinguished into two subgroups by their carboxy-terminal amino acids, leucine, or methionine. Consequently, the enkephalins are either classify as met-encephalins and leu-encephalins, respectively:
- The met-enkephalinspresent the amino acid sequence Tyr-Gly-Gly-Phe-Met.
- The leu-enkephalinspresent the amino acid sequence Tyr-Gly-Gly-Phe-Leu.
Enkephalin peptides act as neurotransmitters and neuromodulators throughout the nervous system and various end-organ targets.[i] Additionally, research has found that met-enkephalin has an essential role in cell proliferation and tissue organization during development.
Early Development of Enkephalins
During the 1980s, researchers discovered that the endogenous opioid system, and met-enkephalin, in particular, has a role in regulating cell proliferation in both normal and neoplastic cell lines. Met-enkephalin, in this context, has the name OGF, and its target receptor is the OGF receptor (OGFr). Notably, OGFr is significantly different in its structure and molecular composition as compared to the classical mu, delta, and kappa opioid receptors. The principal mechanism of action is through the upregulation of p16 and p21 cyclin-dependent kinases, which serve to stall the progression of the cell replication cycle from the G0/G1 phase to the S phase. The system is tonically active, and OGFr protein and gene expression are present in most proliferating cell lines.[9]
Organ systems involved include:
- Nervous systems – CNS, PNS, ANS
- Cardiac systems
- Respiratory system
- Gastrointestinal system
- Endocrine system
- Immune system
Function of Enkephalins[ii]
The expression of enkephalins and their target opioid receptors have a wide distribution throughout the central, peripheral, and autonomic nervous systems, multiple organ systems, as well as endocrine tissues and their target organs. The various effects of enkephalins are best understood by considering a small sample of these experimentally studied systems. The extensive literature on enkephalins physiological effects includes but is not limited to its role in analgesia, angiogenesis, blood pressure regulation, embryonic development, feeding, hypoxia, limbic system modulation (emotional conditions), memory processes, neuroprotection, peristalsis, pancreatic secretion, wound repair, respiratory control, and hepatoprotective mechanisms. Again, leu-enkephalin seems to be involved in the control of the gonadal function. The main functions concern analgesia, stress response regulation, and peristalsis modulation.
Functions include:
- Analgesia
- Stress response regulation (improves release of corticotropin-releasing factor (CRF))
- Peristalsis – slow GI motility by alerting neuronal excitability
Mechanisms[iii]
Enkephalins exert their physiological effect through specific opioid receptors, which have a broad distribution in the body. Three major classes of opioid receptors exist and are named mu (mainly expressed in the CNS), delta (equally expressed in the SNC and spinal cord), and kappa (expressed primarily in the spinal cord). The fourth class of opioid receptors called nociceptin was discovered in 1994 but is not considered to be part of the aforementioned tripartite group, which is often referred to as the classical opioid receptors.
Enkephalins have the highest affinity for the delta-opioid receptor, followed by the mu-opioid receptor, and exhibit low affinity for the kappa-opioid receptor.
Opioid receptors are in the family of G-protein coupled receptors recognized by their seven membrane-spanning motifs with approximately 60% sequence homology. Their extracellular domains, which determine their selectivity, reported between 34 to 49% when comparing sequence similarity. The significant inhibitory effects of enkephalins are mediated by reducing K+ and Ca2+ influx. Signal transduction begins with ligand binding, which causes dissociation of the Gα and Gβγ subunits. The Gα subunit directly interacts with inward rectifying potassium channels causing cellular hyperpolarization. The Gα subunit also inhibits adenylyl cyclase activity, which decreases the formation of cAMP, thus reducing the cAMP-dependent Ca2+ influx. The Gβγ further reduces calcium influx by directly binding to various classes of Ca2+ channels.
Drug Abuse
The role of the endogenous enkephalinergic system (e.g., enkephalin peptides and receptors they bind to) in modulating the reward pathway and reward-related behaviors because (1) there is widespread synthesis and release of enkephalins in the reward pathway and (2) the receptor targets of enkephalin are also widely distributed throughout the reward circuitry, namely the mesolimbic and nigrostriatal pathways.[iv] Enkephalins can potentially be used for substance or other reward-based addictions.
Met-Enkephalin (MENK)
Methionine enkephalin (Met-enkephalin, MENK or Met-enk), was originally discovered by Hughes in 1975.[v] It is an endogenous opioid, derived from pre-enkephalin and has the amino acid sequence of Tyr-Gly-Gly-Phe-Met. MENK is found in the blood at low concentrations and is present in all parts of the nervous system. Studies into the neuroanatomic relationship of MENK have reported higher levels of MENK in the caudate nucleus, globus pallidus, putamen and substantia nigra by radioimmunoassay. As a member of the endogenous opiate family, MENK is well-known as a long-lasting analgesic, and has an important role in modulating pain sensitivity.[vi]
There are increasing numbers of reports supporting the observation that MENK, is involved in a regulatory loop between the neuroendocrine and immune systems and has an immune modulatory role.
Met-Enkephalin and Immunity
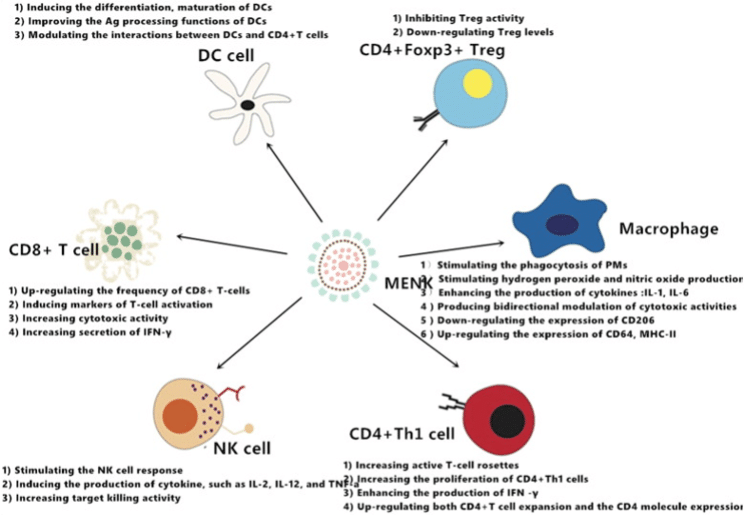
Met-enkephalin (MENK), an endogenous neuropeptide has a crucial role in both neuroendocrine and immune systems.[vii] MENK is believed to have an immunoregulatory activity to have cancer biotherapy activity by binding to the opioid receptors on immune and cancer cells. Clinical studies in cancer patients have reported that MENK activates immune cells directly and by inhibiting regulatory T-cells (Tregs).[viii] MENK may also change the tumor microenvironment by binding to opioid receptor on or in cancer cells. All of these mechanisms of action have biologic significance and potential for use in cancer immunotherapy. Furthermore, they reveal a relationship between the endocrine and immune systems. Due to the apparent role of MENK in cancer therapy we reviewed herein, the research undertaken with MENK in recent years; which has advanced our understanding of the role MENK has in cancer progression and its relationship to immunity, supporting MENK as a new strategy for cancer immunotherapy.
MENK has been reported to exert anti-influenza virus activity by regulating innate immunity in vivo and in vitro. A 2023 study reported pulmonary delivery of MENK via intranasal administration reduced viral titres, upregulated opioid receptor MOR and DOR, increased the proportions of T-cell subsets including CD8+ T cells, CD8+ TEM cells, NP/PA-effector CD8+ TEM cells in bronchoalveolar lavage fluid and lungs, and CD4+/CD8+ TCM cells in lymph nodes to protect mice against influenza viral challenge.[ix] Furthermore, we demonstrated that, on the 10th day of infection, the proportions of CD4+ TM and CD8+ TM cells were significantly increased, which meant that a stable TCM and TEM lineage was established in the early stage of influenza infection.
Preclinical studies have warranted Phase I and Phase II clinical trials using met-enkephalin infusions as a treatment for patients with advanced, unresectable pancreatic cancers. Met-enkephalin is reported in studies to utilize the OGF-OGFr axis to mediate pancreatic tumor progression.[x]
Clinical trials to assess Met-enkephalin treatment of advanced pancreatic cancer were conducted by Zagon et al and Smith et al at The Pennsylvania State University College of Medicine.[xi],[xii] The maximum tolerated dose (MTD) was established at 250 μg/kg infused over a period of 30 min. Patients with unresectable advanced pancreatic adenocarcinoma were treated with the MTD to establish safety and toxicity. No adverse effects related to cardiac rhythm, blood values, neurological status or other laboratory tests were reported; hypotension was the dose-limiting toxicity. Mean survival time for the patients in the study, including those receiving only one dosage of Met-enkephalin, was over 8.5 mo, and two patients had resolution of liver metastases. These observations support further clinical trials on Met-enkephalin as a treatment of advanced pancreatic cancer.
A prospective phase Ⅱ open-labeled clinical trial with 24 patients who failed standard chemotherapy for advanced pancreatic cancer was conducted whereby patients were treated weekly with 250 μg/kg Met-enkephalin by intravenous infusion.[xiii] Outcomes were tumor size measured by computer tomography, survival time, and quality of life. Blood samples were evaluated for levels of Met-enkephalin after 4 and 8 wk of infusion. Data on the Met-enkephalin treatment were compared to results obtained from a control group (n-166) of patients of equivalent age who failed therapy and were discharged to hospice care. Met-enkephalin -treated patients had a three-fold increase in median survival time in comparison to untreated patients. Tumor size was stabilized or reduced in 62% of the cancer patients receiving Met-enkephalin and surviving more than 8 wk in order to conduct the tomography. Plasma enkephalin levels were significantly increased at 4 and 8 wk with blood levels reaching approximate 55 pg/ml in comparison to baseline values of 8 pg/ml. Finally, no adverse effects on blood chemistry were noted, confirming the safety and lack of toxicity of Met-enkephalin. Feedback from patients receiving Met-enkephalin and their caregivers on quality of life indicated that Met-enkephalin infusion did not indicate any stress or pain.
Metabolic Support – Weight Management
Opioid growth factor receptor (Ogfr) is highly expressed in adipocytes and are reported to promote thermogenesis.[xiv] At the cellular level, OGFr enhanced the production of mitochondrial trifunctional protein subunit α (MTPα) and also interacted with MTPα, thus promoting fatty acid oxidation. OGFr is reported important in fatty acid metabolism and adipose thermogenesis.